Shoulder Osteoarthritis
Specialist Physiotherapy for Glenohumeral Joint Arthritis
Book an appointmentShoulder Osteoarthritis
Shoulder osteoarthritis is less common than hip or knee arthritis, but when it develops it can significantly affect comfort, sleep and overhead function.
Unlike weight-bearing joints, the shoulder is designed primarily for mobility. It sacrifices stability for range. When osteoarthritis affects the glenohumeral joint, that mobility often becomes restricted and painful, particularly during reaching, lifting or movements above shoulder height.
Many people first notice stiffness when putting on a coat, fastening a bra, reaching into a back seat or lifting something into a cupboard. Others are troubled more by night pain, especially when lying on the affected side.
Although commonly described as “wear and tear,” shoulder osteoarthritis is better understood as a long-term adaptive process within a joint that has been used extensively over decades. Structural change alone does not explain the full experience of pain. Muscle function, joint loading patterns, inflammation during flares and nervous system sensitivity all contribute to symptoms.
A broader understanding leads to more intelligent management.

What Actually Happens in Shoulder Osteoarthritis?
The glenohumeral joint is a ball-and-socket joint between the humeral head and the glenoid of the scapula. It relies heavily on surrounding musculature, particularly the rotator cuff, for dynamic stability.
In osteoarthritis, cartilage surfaces gradually change. The body may respond by forming osteophytes and altering joint contour. Over time, joint space may narrow and movement becomes less fluid.
However, imaging findings do not consistently predict symptom severity. Some individuals with clear radiographic change function well. Others with modest structural findings experience significant restriction and pain.
Clinical decisions should therefore be guided by symptoms and functional impact rather than scan language alone.
How Shoulder Osteoarthritis Commonly Presents
Pain is typically felt deep within the shoulder joint. It may radiate into the upper arm but rarely below the elbow. Stiffness is a dominant feature. External rotation and elevation are often the first movements to become restricted.
Night pain is common and can be one of the most distressing aspects of the condition. Lying on the affected side or sustaining one position for prolonged periods may increase discomfort.
During flare episodes, the shoulder may feel more irritable and reactive to movements that are normally tolerable. These flares often follow increased activity, overhead work, decorating, gardening or a change in exercise routine.
Importantly, a flare does not usually mean rapid deterioration. It more commonly reflects temporary joint sensitivity.
Movement and Load
A frequent concern is whether continued movement will accelerate joint damage.
Appropriately graded activity does not worsen osteoarthritis. In fact, maintaining movement is critical to preserving shoulder function. Avoidance leads to progressive stiffness, reduced rotator cuff support and increased vulnerability.
Rehabilitation focuses on restoring range where possible, strengthening dynamic stabilisers and improving tolerance to overhead and functional tasks.
The objective is not to eliminate all discomfort immediately, but to maintain independence and prevent progressive functional decline.
Flare Management
Shoulder osteoarthritis tends to fluctuate.
During a flare, the goal is temporary modification rather than immobilisation. Sustained rest often increases stiffness. Reducing provocative loading, maintaining gentle mobility and gradually reintroducing strengthening once irritability settles helps shorten flare duration.
Calm, informed management reduces fear and prevents overcorrection.
Imaging: When Is It Necessary?
A clinical assessment is often sufficient to diagnose shoulder osteoarthritis. The pattern of stiffness, movement restriction and symptom behaviour typically provides clear diagnostic direction.
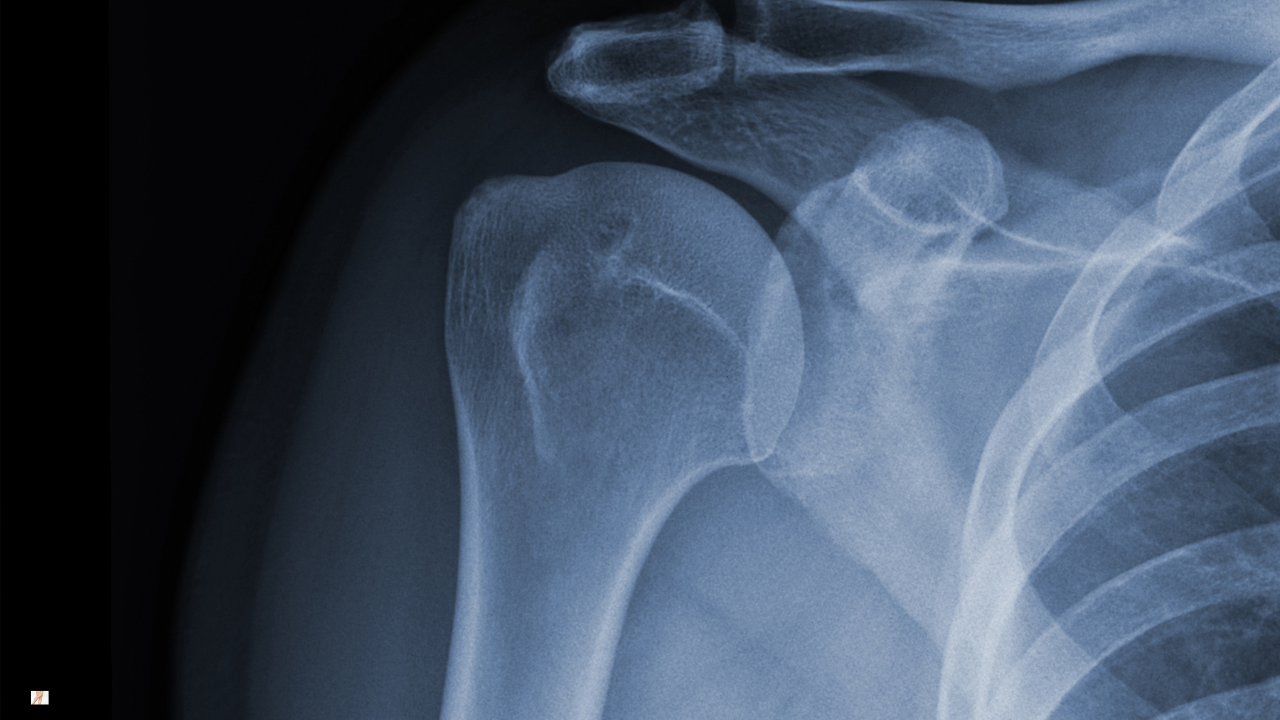
Plain X-ray can confirm structural joint change and may show joint space narrowing, osteophyte formation or altered joint contour. However, the presence of these findings does not automatically determine symptom severity or treatment pathway.
MRI is rarely required unless symptoms suggest additional pathology such as significant rotator cuff tear, instability or atypical presentation. In many cases, MRI findings can create confusion rather than clarity, as age-related changes in the shoulder are common even in individuals without pain.
Imaging is most useful when surgical options are being considered, when symptoms do not follow an expected pattern, or when there is uncertainty about diagnosis.
Treatment decisions should be guided primarily by function, symptom impact and clinical assessment — not scan language alone.
Injection Therapy for Shoulder Osteoarthritis
Corticosteroid injection into the glenohumeral joint may provide temporary symptom relief in selected individuals, particularly where pain limits rehabilitation or sleep.
Relief duration varies. Injections do not reverse structural change. Their role is to reduce inflammation and create a window for meaningful strengthening and functional progress.
Injection decisions should form part of a structured management plan rather than replace rehabilitation.
When Is Shoulder Replacement Appropriate?
Shoulder replacement surgery may be appropriate when pain and functional restriction remain severe despite comprehensive conservative care.
Unlike hip replacement, shoulder arthroplasty is less common and requires careful selection. Outcomes can be excellent in appropriately indicated cases, particularly where joint surfaces are significantly degenerated and quality of life is compromised.
However, surgery is rarely urgent. Many individuals manage symptoms effectively for years with structured physiotherapy and load management.
Shared decision-making is central. The decision should be guided by symptom severity, lifestyle demands and informed discussion of realistic outcomes.
Our Specialist Approach to Shoulder Osteoarthritis
Assessment focuses on movement restriction, rotator cuff function, load tolerance and symptom behaviour.
Management emphasises progressive strengthening, mobility restoration where possible, intelligent load planning and flare guidance. Where appropriate, we discuss injection options and surgical referral pathways.
The aim is to preserve functional range, maintain strength and support confident use of the arm in everyday life.
Understanding Osteoarthritis
Shoulder osteoarthritis is one part of our wider specialist osteoarthritis service. For a broader understanding of how osteoarthritis develops and how structured rehabilitation supports long-term joint health, you can explore our main osteoarthritis overview page.
Learn More About OsteoarthritisFrequently Asked Questions About Shoulder Osteoarthritis
Is shoulder stiffness always arthritis?
Why is my shoulder worse at night?
Will continuing to use my arm cause more damage?
Does shoulder osteoarthritis inevitably progress?
When should I consider an injection?
Is shoulder replacement inevitable?
Book a Specialist Shoulder Assessment
If shoulder osteoarthritis is affecting your mobility, confidence or quality of life, appointments are available within our specialist clinics. Assessment focuses on restoring strength, managing flare-ups and guiding informed decisions about long-term care.
Appointments for shoulder osteoarthritis are available within our specialist clinic in Fareham.
Book Your Shoulder Assessment
